The Fine Print
In the Army's separations manual it's called Regulation 635-200, Chapter 5-13: "Separation Because of Personality Disorder." It's an alluring choice for a cash-strapped military because enacting it is quick and cheap. The Department of Veterans Affairs doesn't have to provide medical care to soldiers dismissed with personality disorder. That's because under Chapter 5-13, personality disorder is a pre-existing condition. The VA is only required to treat wounds sustained during service.
Soldiers discharged under 5-13 can't collect disability pay either. To receive those benefits, a soldier must be evaluated by a medical board, which must confirm that he is wounded and that his wounds stem from combat. The process takes several months, in contrast with a 5-13 discharge, which can be wrapped up in a few days.
If a soldier dismissed under 5-13 hasn't served out his contract, he has to give back a slice of his re-enlistment bonus as well. That amount is often larger than the soldier's final paycheck. As a result, on the day of their discharge, many injured vets learn that they owe the Army several thousand dollars.
 One military official says doctors at his base are doing more than withholding this information from wounded soldiers; they're actually telling them the opposite: that if they go along with a 5-13, they'll get to keep their bonus and receive disability and medical benefits. The official, who demanded anonymity, handles discharge papers at a prominent Army facility. He says the soldiers he works with know they don't have a personality disorder. "But the doctors are telling them, this will get you out quicker, and the VA will take care of you. To stay out of Iraq, a soldier will take that in a heartbeat. What they don't realize is, those things are lies. The soldiers, they don't read the fine print," he says. "They don't know to ask for a med board. They're taking the word of the doctors. Then they sit down with me and find out what a 5-13 really means—they're shocked." One military official says doctors at his base are doing more than withholding this information from wounded soldiers; they're actually telling them the opposite: that if they go along with a 5-13, they'll get to keep their bonus and receive disability and medical benefits. The official, who demanded anonymity, handles discharge papers at a prominent Army facility. He says the soldiers he works with know they don't have a personality disorder. "But the doctors are telling them, this will get you out quicker, and the VA will take care of you. To stay out of Iraq, a soldier will take that in a heartbeat. What they don't realize is, those things are lies. The soldiers, they don't read the fine print," he says. "They don't know to ask for a med board. They're taking the word of the doctors. Then they sit down with me and find out what a 5-13 really means—they're shocked."
Russell Terry, founder of the Iraq War Veterans Organization (IWVO), says he's watched this scenario play itself out many times. For more than a year, his veterans' rights group has been receiving calls from distraught soldiers discharged under Chapter 5-13. Most, he says, say their military doctors pushed the personality disorder diagnosis, strained to prove that their problems existed before their service in Iraq and refused to acknowledge evidence of posttraumatic stress disorder (PTSD), traumatic brain injury and physical traumas, which would allow them to collect disability and medical benefits.
"These soldiers are coming home from Iraq with all kinds of problems," Terry says. "They go to the VA for treatment, and they're turned away. They're told, 'No, you have a pre-existing condition, something from childhood.'" That leap in logic boils Terry's blood. "Everybody receives a psychological screening when they join the military. What I want to know is, if all these soldiers really did have a severe pre-existing condition, how did they get into the military in the first place?"
Terry says that trying to reverse a 5-13 discharge is a frustrating process. A soldier has to claw through a thicket of paperwork, appeals panels and backstage political dealing, and even with the guidance of an experienced advocate, few are successful. "The 5-13," he says, "it's like a scarlet letter you can't get taken off."
In the last six years the Army has diagnosed and discharged more than 5,600 soldiers because of personality disorder, according to the Defense Department. And the numbers keep rising: 805 cases in 2001, 980 cases in 2003, 1,086 from January to November 2006. "It's getting worse and worse every day," says the official who handles discharge papers. "At my office the numbers started out normal. Now it's up to three or four soldiers each day. It's like, suddenly everybody has a personality disorder."
The reason is simple, he says. "They're saving a buck. And they're saving the VA money too. It's all about money."
Exactly how much money is difficult to calculate. Defense Department records show that across the entire armed forces, more than 22,500 soldiers have been dismissed due to personality disorder in the last six years. How much those soldiers would have collected in disability pay would have been determined by a medical board, which evaluates just how disabled a veteran is. A completely disabled soldier receives about $44,000 a year. In a recent study on the cost of veterans' benefits for the Iraq and Afghanistan wars, Harvard professor Linda Bilmes estimates an average disability payout of $8,890 per year and a future life expectancy of forty years for soldiers returning from service.
Using those figures, by discharging soldiers under Chapter 5-13, the military could be saving upwards of $8 billion in disability pay. Add to that savings the cost of medical care over the soldiers' lifetimes. Bilmes estimates that each year the VA spends an average of $5,000 in medical care per veteran. Applying those numbers, by discharging 22,500 soldiers because of personality disorder, the military saves $4.5 billion in medical care over their lifetimes.
Town says Fort Carson psychologist Mark Wexler assured him that he would receive disability benefits, VA medical care and that he'd get to keep his bonus—good news he discussed with Christian Fields and Brandon Murray, two soldiers in his unit at Fort Carson. "We talked about it many times," Murray says. "Jon said the doctor there promised him benefits, and he was happy about it. Who wouldn't be?" Town shared that excitement with his wife, Kristy, shortly after his appointment with Wexler. "He said that Wexler had explained to him that he'd get to keep his benefits," Kristy says, "that the doctor had looked into it, and it was all coming with the chapter he was getting."
In fact, Town would not get disability pay or receive long-term VA medical care. And he would have to give back the bulk of his $15,000 bonus. Returning that money meant Town would leave Fort Carson less than empty-handed: He now owed the Army more than $3,000. "We had this on our heads the whole way, driving home to Ohio," says Town. Wexler made him promises, he says, about what would happen if he went along with the diagnosis. "The final day, we find out, none of it was true. It was a total shock. I felt like I'd been betrayed by the Army."
Wexler denies discussing benefits with Town. In a statement, the psychologist writes, "I have never discussed benefits with my patients as that is not my area of expertise. The only thing I said to Spc. Town was that the Chapter 5-13 is an honorable discharge.... I assure you, after over 15 years in my position, both as active duty and now civilian, I don't presume to know all the details about benefits and therefore do not discuss them with my patients."
Wexler's boss, Col. Steven Knorr, chief of the Department of Behavioral Health at Evans Army Hospital, declined to speak about Town's case. When asked if doctors at Fort Carson were assuring patients set for a 5-13 discharge that they'll receive disability benefits and keep their bonuses, Knorr said, "I don't believe they're doing that."
'Not the Man He Used to Be'
Interviews with soldiers diagnosed with personality disorder suggest that the military is using the psychological condition as a catch-all diagnosis, encompassing symptoms as diverse as deafness, headaches and schizophrenic delusions. That flies in the face of the Army's own regulations.
According to those regulations, to be classified a personality disorder, a soldier's symptoms had to exist before he joined the military. And they have to match the "personality disorder" described in the Diagnostic and Statistical Manual of Mental Disorders, the national standard for psychiatric diagnosis. Town's case provides a clear window into how these personality disorder diagnoses are being used because even a cursory examination of his case casts grave doubt as to whether he fits either criterion.
Town's wife, for one, laughs in disbelief at the idea that her husband was suffering from hearing loss before he headed to Iraq. But since returning, she says, he can't watch TV unless the volume is full-blast, can't use the phone unless its volume is set to high. Medical papers from Fort Carson list Town as having no health problems before serving in Iraq; after, a Fort Carson audiologist documents "functional (non-organic) hearing loss." Town says his right ear, his "good" ear, has lost 50 percent of its hearing; his left is still essentially useless.
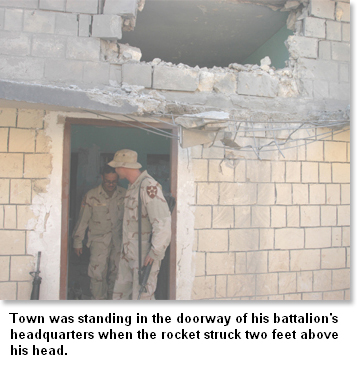
He is more disturbed by how his memory has eroded. Since the rocket blast, he has struggled to retain new information. "Like, I'll be driving places, and then I totally forget where I'm going," he says. "Numbers, names, dates—unless I knew them before, I pretty much don't remember." When Town returned to his desk job at Fort Carson, he found himself straining to recall the Army's regulations. "People were like, 'What are you, dumb?' And I'm like, 'No, I'm probably smarter than you. I just can't remember stuff,'" he says, his melancholy suddenly replaced by anger. "They don't understand—I got hit by a rocket."
Those bursts of rage mark the biggest change, says Kristy Town. She says the man she married four years ago was "a real goofball. He'd do funny voices and faces—a great Jim Carrey imitation. When the kids would get a boo-boo, he'd fall on the ground and pretend he got a boo-boo too." Now, she says, "his emotions are all over the place. He'll get so angry at things, and it's not toward anybody. It's toward himself. He blames himself for everything." He has a hard time sleeping and doesn't spend as much time as he used to with the kids. "They get rowdy when they play, and he just has to be alone. It's almost like his nerves can't handle it."
Kristy begins to cry, pauses, before forcing herself to continue. She's been watching him when he's alone, she says. "He kind of... zones out, almost like he's in a daze."
In May 2006 Town tried to electrocute himself, dropping his wife's hair dryer into the bathtub. The dryer short-circuited before it could electrify the water. Fort Carson officials put Town in an off-post hospital that specializes in suicidal depression. Town had been promoted to corporal after returning from Iraq; he was stripped of that rank and reduced back to specialist. "When he came back, I tried to be the same," Kristy says. "He just can't. He's definitely not the man he used to be."
Town says his dreams have changed too. They keep taking him back to Ramadi, to the death of a good friend who'd been too near an explosion, taken too much shrapnel to the face. In his dreams Town returns there night after night to soak up the blood.
He stops his description for a rare moment of levity. "Sleep didn't use to be like that," he says. "I used to sleep just fine."
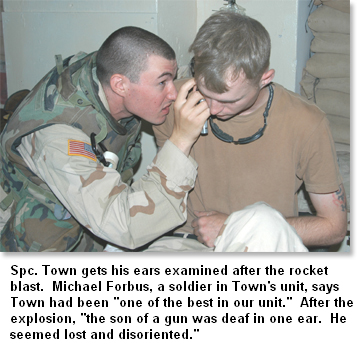
How the Army determined then that Town's behavioral problems existed before his military service is unclear. Wexler, the Fort Carson psychologist who made the diagnosis, didn't interview any of Town's family or friends. It's unclear whether he even questioned Town's fellow soldiers in 2-17 Field Artillery, men like Fields, Murray and Michael Forbus, who could have testified to his stability and award-winning performance before the October 2004 rocket attack. As Forbus puts it, before the attack Town was "one of the best in our unit"; after, "the son of a gun was deaf in one ear. He seemed lost and disoriented. It just took the life out of him."
Town finds his diagnosis especially strange because the Diagnostic Manual appears to preclude cases like his. It says that a pattern of erratic behavior cannot be labeled a "personality disorder" if it's from a head injury. The specialist asserts that his hearing loss, headaches and anger all began with the rocket attack that knocked him unconscious.
Wexler did not reply to repeated requests seeking comment on Town's diagnosis. But Col. Knorr of Fort Carson's Evans hospital says he's confident his doctors are properly diagnosing personality disorder. The colonel says there is a simple explanation as to why in so many cases the lifelong condition of personality disorder isn't apparent until after serving in Iraq. Traumatic experiences, Knorr says, can trigger a condition that has lain dormant for years. "They may have done fine in high school and before, but it comes out during the stress of service."
"I've never heard of that occurring," says Keith Armstrong, a clinical professor with the Department of Psychiatry at the University of California, San Francisco. Armstrong has been counseling traumatized veterans for more than twenty years at the San Francisco VA; most recently he is the co-author of Courage After Fire: Coping Strategies for Troops Returning From Iraq and Afghanistan and Their Families. "Personality disorder is a diagnosis I'm very cautious about," he says. "My question would be, has PTSD been ruled out? It seems to me that if it walks like a duck, looks like a duck, let's see if it's a duck before other factors are implicated."
Knorr admits that in most cases, before making a diagnosis, his doctors only interview the soldier. But he adds that interviewing family members, untrained to recognize signs of personality disorder, would be of limited value. "The soldier's perception and their parents' perception is that they were fine. But maybe they didn't or weren't able to see that wasn't the case."
 Armstrong takes a very different approach. He says family is a "crucial part" of the diagnosis and treatment of soldiers returning from war. The professor sees parents and wives as so important, he encourages his soldiers to invite their families into the counseling sessions. "They bring in particular information that can be helpful," he says. "By not taking advantage of their knowledge and support, I think we're doing soldiers a disservice." Armstrong takes a very different approach. He says family is a "crucial part" of the diagnosis and treatment of soldiers returning from war. The professor sees parents and wives as so important, he encourages his soldiers to invite their families into the counseling sessions. "They bring in particular information that can be helpful," he says. "By not taking advantage of their knowledge and support, I think we're doing soldiers a disservice."
Knorr would not discuss the specifics of Town's case. He did note, however, that his department treats thousands of soldiers each year and says within that population, there are bound to be a small fraction of misdiagnosed cases and dissatisfied soldiers. He adds that the soldiers he's seen diagnosed and discharged with personality disorder are "usually quite pleased."
The Army holds soldiers' medical records and contact information strictly confidential. But The Nation was able to locate a half-dozen soldiers from bases across the country who were diagnosed with personality disorder. All of them rejected that diagnosis. Most said military doctors tried to force the diagnosis upon them and turned a blind eye to symptoms of PTSD and physical injury.
One such veteran, Richard Dykstra, went to the hospital at Fort Stewart, Georgia, complaining of flashbacks, anger and stomach pains. The doctor there diagnosed personality disorder. Dykstra thinks the symptoms actually stem from PTSD and a bilateral hernia he suffered in Iraq. "When I told her my symptoms, she said, 'Oh, it looks like you've been reading up on PTSD.' Then she basically said I was making it all up," he says.
In her report on Dykstra, Col. Ana Parodi, head of Behavioral Health at Fort Stewart's Winn Army Hospital, writes that the soldier gives a clear description of PTSD symptoms but lays them out with such detail, it's "as if he had memorized the criteria." She concludes that Dykstra has personality disorder, not PTSD, though her report also notes that Dykstra has had "no previous psychiatric history" and that she confirmed the validity of his symptoms with the soldier's wife.
Parodi is currently on leave and could not be reached for comment. Speaking for Fort Stewart, Public Affairs Officer Lieut. Col. Randy Martin says that the Army's diagnosis procedures "have been developed over time, and they are accepted as being fair." Martin said he could not address Dykstra's case specifically because his files have been moved to a storage facility in St. Louis.
William Wooldridge had a similar fight with the Army. The specialist was hauling missiles and tank ammunition outside Baghdad when, he says, a man standing at the side of the road grabbed hold of a young girl and pushed her in front of his truck. "The little girl," Wooldridge says, his voice suddenly quiet, "she looked like one of my daughters."
When he returned to Fort Polk, Louisiana, Wooldridge told his doctor that he was now hearing voices and seeing visions, hallucinations of a mangled girl who would ask him why he had killed her. His doctor told him he had personality disorder. "When I heard that, I flew off the handle because I said, 'Hey, that ain't me. Before I went over there, I was a happy-go-lucky kind of guy.'" Wooldridge says his psychologist, Capt. Patrick Brady of Baynes-Jones Army Community Hospital, saw him for thirty minutes before making his diagnosis. Soon after, Wooldridge was discharged from Fort Polk under Chapter 5-13.
He began to fight that discharge immediately, without success. Then in March 2005, eighteen months after Wooldridge's dismissal, his psychiatrist at the Memphis VA filed papers rejecting Brady's diagnosis and asserting that Wooldridge suffered from PTSD so severe, it made him "totally disabled." Weeks later the Army Discharge Review Board voided Wooldridge's 5-13 dismissal, but the eighteen months he'd spent lingering without benefits had already taken its toll.
"They put me out on the street to rot, and if I had left things like they were, there would have been no way I could have survived. I would have had to take myself out or had someone do it for me," he says. The way they use personality disorder to diagnose and discharge, he says, "it's like a mental rape. That's the only way I can describe it."
Captain Brady has since left Fort Polk and is now on staff at Fort Wainwright, Alaska; recently he deployed to Iraq and was unavailable for comment. In a statement, Maj. Byron Strother, chief of the Department of Behavioral Health at Baynes-Jones hospital, writes that allegations that soldiers at Fort Polk are being misdiagnosed "are not true." Strother says diagnoses at his hospital are made "only after careful consideration of all relevant clinical observation, direct examination [and] appropriate testing."
If there are dissatisfied soldiers, says Knorr, the Fort Carson official, "I'll bet not a single one of them has been diagnosed with conditions that are clear-cut and makes them medically unfit, like schizophrenia."
Linda Mosier disputes that. When her son Chris left for Iraq in 2004, he was a "normal kid," she says, who'd call her long-distance and joke about the strange food and expensive taxis overseas. When he returned home for Christmas 2005, "he wouldn't sit down for a meal with us. He just kept walking around. I took him to the department store for slacks, and he was inside rushing around saying, 'Let's go, let's go, let's go.' He wouldn't sleep, and the one time he did, he woke up screaming."
Mosier told his mother of a breaking point in Iraq: a roadside bomb that blew up the truck in front of his. "He said his buddies were screaming. They were on fire," she says, her voice trailing off. "He was there at the end to pick up the hands and arms." After that Mosier started having delusions. Dr. Wexler of Fort Carson diagnosed personality disorder. Soon after, Mosier was discharged under Chapter 5-13.
Mosier returned home, still plagued by visions. In October he put a note on the front door of their Des Moines, Iowa, home saying the Iraqis were after him and he had to protect the family, then shot himself.
Mosier's mother is furious that doctors at Fort Carson treated her son for such a brief period of time and that Wexler, citing confidentiality, refused to tell her anything about that treatment or give her family any direction on how to help Chris upon his return home. She does not believe her son had a personality disorder. "They take a normal kid, he comes back messed up, then nobody was there for him when he came back," Linda says. "They discharged him so they didn't have to treat him."
Wexler did not reply to a written request seeking comment on Mosier's case.
'Thrown to the Wolves'
Today Jon Town is home, in small-town Findlay, Ohio, with no job, no prospects and plenty of time to reflect on how he got there. Diagnosing him with personality disorder may have saved the Army thousands of dollars, he says, but what did Wexler have to gain?
 Quite a lot, says Steve Robinson, director of veterans affairs at Veterans for America, a Washington, DC-based soldiers' rights group. Since the Iraq War began, he says, doctors have been facing an overflow of wounded soldiers and a shortage of rooms, supplies and time to treat them. By calling PTSD a personality disorder, they usher one soldier out quickly, freeing up space for the three or four who are waiting. Quite a lot, says Steve Robinson, director of veterans affairs at Veterans for America, a Washington, DC-based soldiers' rights group. Since the Iraq War began, he says, doctors have been facing an overflow of wounded soldiers and a shortage of rooms, supplies and time to treat them. By calling PTSD a personality disorder, they usher one soldier out quickly, freeing up space for the three or four who are waiting.
Terry, the veterans' advocate from IWVO, notes that unlike doctors in the private sector, Army doctors who give questionable diagnoses face no danger of malpractice suits due to Feres v. U.S., a 1950 Supreme Court ruling that bars soldiers from suing for negligence. To maintain that protection, Terry says, most doctors will diagnose personality disorder when prodded to do so by military officials.
That's precisely how the system works, says one military official familiar with the discharge process. The official, who requested anonymity, is a lawyer with Trial Defense Services (TDS), a unit of the Army that guides soldiers through their 5-13 discharge. "Commanders want to get these guys out the door and get it done fast. Even if the next soldier isn't as good, at least he's good to go. He's deployable. So they're telling the docs what diagnosis to give to get what discharge."
The lawyer says he knows this is happening because commanders have told him that they're doing it. "Some have come to me and talked about doing this. They're saying, 'Give me a specific diagnosis. It'll support a certain chapter.'"
Colonel Martin of Fort Stewart said the prospect of commanders pressuring doctors to diagnose personality disorder is "highly unlikely." "Doctors are making these determinations themselves," Martin says. In a statement, Col. William Statz, commander at Fort Polk's Baynes-Jones hospital, says, "Any allegations that clinical decisions are influenced by either political considerations or command pressures, at any level, are untrue."
But a second TDS lawyer, who also demanded anonymity, says he's watched the same process play out at his base. "What I've noticed is right before a unit deploys, we see a spike in 5-13s, as if the commanders are trying to clean house, get rid of the soldiers they don't really need," he says. "The chain of command just wants to eliminate them and get a new body in there fast to plug up the holes." If anyone shows even moderate signs of psychological distress, he says, "they're kicking them to the curb instead of treating them."
Both lawyers say that once a commander steps in and pushes for a 5-13, the diagnosis and discharge are carved in stone fairly fast. After that happens, one lawyer says he points soldiers toward the Army Board for Correction of Military Records, where a 5-13 label could be overturned, and failing that, advises them to seek redress from their representative in Congress. Town did that, contacting Republican Representative Michael Oxley of Ohio, with little success. Oxley, who has since retired, did not return calls seeking comment.
Few cases are challenged successfully or overturned later, say the TDS lawyers. The system, says one, is essentially broken. "Right now, the Army is eating its own. What I want to see is these soldiers getting the right diagnosis, so they can get the right help, not be thrown to the wolves right away. That is what they're doing."
Still, Town tries to remain undaunted. He got his story to Robinson of Veterans for America, who brought papers on his case to an October meeting with several top Washington officials, including Deputy Surgeon General Gale Pollock, Assistant Surgeon General Bernard DeKoning and Republican Senator Kit Bond of Missouri. There Robinson laid out the larger 5-13 problem and submitted a briefing specifically on Town.
"We got a very positive response," Robinson says. "After we presented, they were almost appalled, like we are every day. They said, 'We didn't know this was happening.'" Robinson says the deputy surgeon general promised to look into Town's case and the others presented to her. Senator Bond, whose son has served in Iraq, floated the idea of a Congressional hearing if the 5-13 issue isn't resolved. The senator did not return calls seeking comment.
In the meantime, Town is doing his best to keep his head in check. He says his nightmares have been waning in recent weeks, but most of his problems persist. He's thinking of going to a veterans support group in Toledo, forty-five miles north of Findlay. There will be guys there who have been through this, he says, vets who understand.
Town hesitates, his voice suddenly much softer. "I have my good days and my bad days," he says. "It all depends on whether I wake up in Findlay or Iraq."
   
|